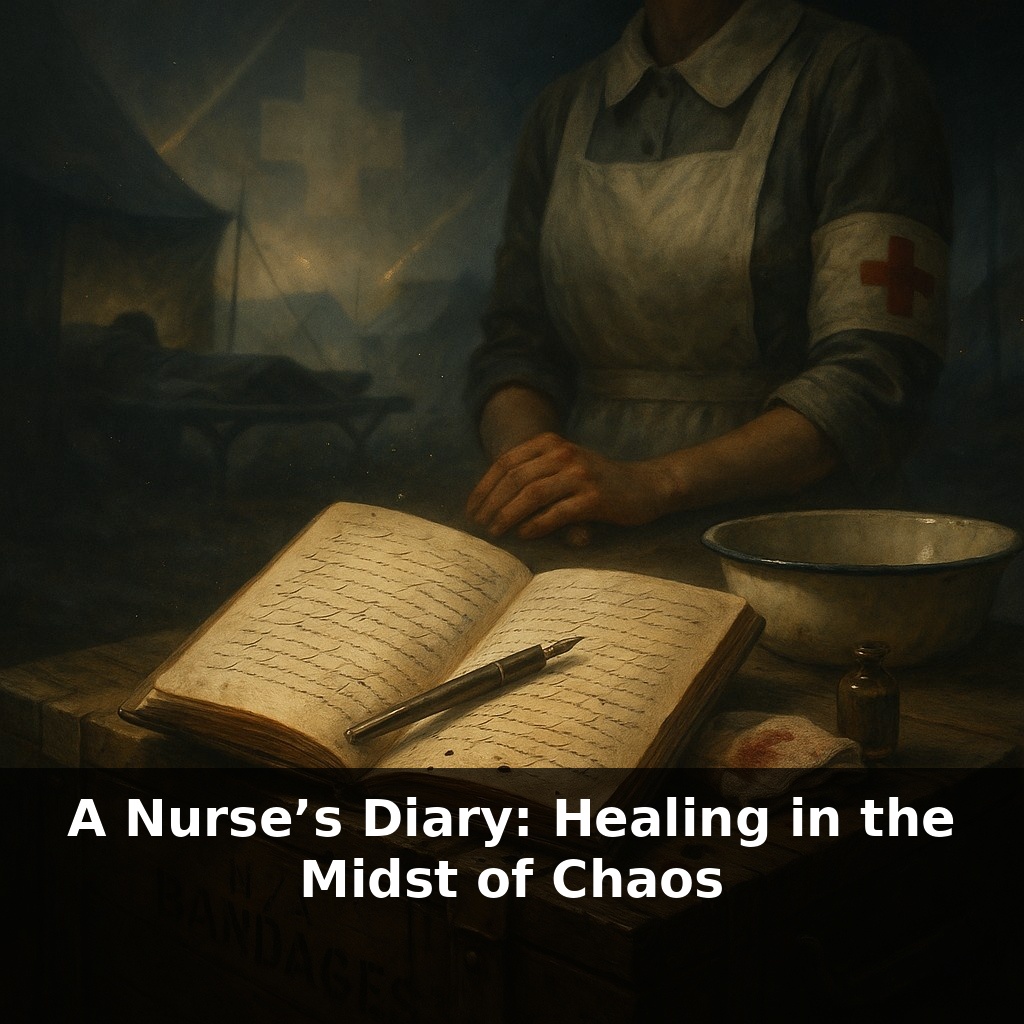
Bombs fall close enough to rattle the enamel basins, yet the nurses keep stitching, dosing, and counting heartbeats. One young lieutenant calculates she’s watched more men slip between life and death in a week than most doctors do in years—and the war has barely begun.
She writes in her diary between siren blasts, ink trembling over paper balanced on a crate of bandages. Today’s entry starts with a smell, not a sight: carbolic, damp canvas, and the metallic tang of blood that never quite leaves her skin. The men arrive in waves—mud-caked, nameless for now, tagged only by the damage war has carved into them. She moves like a conductor through discordant noise, turning chaos into a rough rhythm: cut, clamp, clean, comfort. Pain meds here, plasma there, a whispered joke to the boy who won’t meet her eyes. Outside, trucks grind gears and guns thud in the distance; inside, time shrinks to the space between pulses under her fingertips. She’s twenty-three, from Ohio, and tonight she’ll improvise an IV stand from a bent rifle, then write it down so she doesn’t forget how, in case tomorrow is worse.
By August 1944, she’s not just treating casualties; she’s helping run a traveling organism that eats fuel, bandages, and blood faster than supply trucks can feed it. Orders pinball down the tent rows: “Surgical team 2, stand by. New convoy, mostly shrapnel, some burns.” Penicillin vials clink in her pocket—precious, rationed, drawn up with the care of pouring the last clean water in a drought. Her mind now tracks numbers like a second heartbeat: units of plasma left, hours since the last sleep, how many beds must be cleared before dawn because the front is moving again, and the wounded follow it like a tide.
They start calling her “Lieutenant Stat” because she is always moving—bed to bed, tent to tent, crisis to crisis. But what looks like frantic motion is actually choreography learned the hard way. In the first weeks she panicked over every groan; now she reads a tent at a glance the way a farmer reads the sky. A shallow breath in cot 3 means hidden chest damage; a certain grayness of lips in cot 7 means blood loss is worse than the chart suggests. No one taught her this in nursing school. The front did.
Her day blurs into layers of decisions. On the surface: dress this burn, change that drip, adjust a dose. Underneath: who is stable enough to wait, who must be pushed to the top of the surgeon’s list, who is too far gone to justify another bottle of scarce blood. The math is brutal and quiet. She will live with some of those choices for the rest of her life.
Statistics filter into camp like rumors. Somewhere above her pay grade, men in pressed uniforms note that abdominal-wound survival is climbing, that infections are dropping. Down here, the translation is simpler: fewer empty beds in the morning. She and her colleagues are the ones wiping, flushing, turning, and rewrapping until pus stays away. No headline will mention that a bored nurse, forced to repeat the same cleaning routine for the hundredth time, is the true enemy of gangrene.
The cast of characters around her keeps changing. Scottish sisters with clipped vowels show her how to rig a ward for cold rain. An exhausted Filipino nurse demonstrates a quicker way to lift a semiconscious man without wrenching her own back. A Black American nurse, kept in a segregated unit, slips over between shifts to trade tricks for calming men in morphine delirium. Their uniforms may be divided on paper, but their methods travel through whispers and borrowed hands.
The hospital itself keeps learning too. One month they start grouping the worst shock cases at the tent nearest the generators, so pumps and lights never flicker when they’re needed most. Another month, someone notices that lining the mud paths with empty crates keeps gurneys from bogging down during rainstorms, shaving minutes off every trip. Small changes, but each one nudges the line between life and death a little farther toward life.
By winter, she realizes she is no longer just following orders; she is co-authoring a playbook no one has written yet. Each shortcut scribbled in her notebook is a seed for some future protocol, far from the guns, in emergencies that haven’t happened yet.
Think of her shift like conducting weather experiments in fast‑forward. Instead of waiting months to see if a new planting method survives the season, she tests a tiny change—raising a cot on ration boxes, warming saline near the stove, clustering the sickest men where she can see all their faces at once—and knows by dawn whether it nudged fevers down or pulses up. Word of what works spreads sideways, not through official memos but through muttered conversations over bad coffee: “Try turning them every hour, not two.” “Don’t bundle the burn dressings so thick; they trap heat.” When a British matron quietly times how long it takes orderlies to find morphine in a cluttered supply tent, the results ripple outward: shelves get labeled, vials grouped by urgency, minutes shaved in the dark. None of this looks like innovation in a lab-coat sense. It is dozens of small, reversible bets, tested under fire, the bedside version of trial and error that will one day harden into checklists no one questions.
Long after the guns fall silent, her “Lieutenant Stat” instincts don’t retire; they migrate. In peacetime disasters—earthquakes, bombings, floods—modern nurses still sort the crush of arrivals, carve order from wreckage, and watch for the small details that tilt outcomes. Their field tricks become today’s modular ICUs, mobile clinics, and mental‑health huddles for staff. Like hardy seeds carried on the wind, those wartime hacks keep sprouting in new emergencies, adapted but recognizable.
Years later, her diary notes outgrow the war, echoed in quiet routines: a nurse taping a family photo to a monitor, another humming off‑key to steady her hands, a third learning a patient’s laugh before their lab values. Like lanterns left along a dark trail, these small, human habits guide new healers through fresh storms no textbook can fully chart.
Before next week, ask yourself: Where in my current shifts do I feel that same “chaos pressure” the nurse described, and what’s one specific boundary (like a timed charting block, a no-phone zone, or a hard stop for staying late) I’m honestly willing to protect this week? When I walk out of work at the end of a brutal day, what’s one tiny ritual—like sitting in the car for two quiet minutes, texting a specific friend, or changing clothes immediately at home—that would help me emotionally “clock out” instead of carrying the unit home with me? During your next really hard patient interaction, what’s one phrase (to yourself or the patient) you can experiment with—such as “I can’t fix everything, but I can be fully present for the next five minutes”—to stay human and compassionate without burning yourself out?